Low blood sugar may sound like a small issue, but for someone living with diabetes — or even certain non-diabetic conditions — it can quickly turn into a medical emergency.
Hypoglycaemia (also spelled hypoglycaemia) refers to a condition where blood glucose levels fall below normal. Glucose is the primary source of energy of body, significantly for the brain. When glucose levels drop too low, the body and brain begin to struggle.
For some people, it causes mild shakiness. For others, it can lead to confusion, unconsciousness, or even seizures. The key difference between a manageable episode and a dangerous one is early recognition and timely action.
Table of Contents
What Is Hypoglycaemia?
It is generally defined as:
- Blood glucose below 70 mg/dL (3.9 mmol/L)
However, symptoms may begin even slightly above this level in some individuals, especially if their body is used to higher glucose levels.
Clinically, it is classified into three levels:
- Level 1: Glucose < 70 mg/dL (warning stage)
- Level 2: Glucose < 54 mg/dL (clinically significant)
- Level 3: Severe hypoglycaemia requiring assistance
The brain depends heavily on glucose. Unlike muscles, it cannot store energy for long. That is why low sugar affects mental function quickly.
Why Does Hypoglycaemia Happen?
1. In People with Diabetes
This is the most common scenario.
- Excess insulin dose
- Skipping meals after taking insulin
- Taking sulfonylureas (like glimepiride)
- Delayed meals
- Intense exercise without adjustment
- Alcohol consumption
Insulin lowers blood sugar. If too much insulin is present compared to available glucose, sugar levels fall rapidly.
2. In Non-Diabetic Individuals
Less common but possible:
- Prolonged fasting
- Severe infections
- Liver disease
- Hormonal deficiencies (e.g., adrenal insufficiency)
- Rare insulin-producing tumors (insulinoma)
Early Warning Signs: Listen to Your Body
The body gives signals before things get severe. These early symptoms occur due to activation of stress hormones like adrenaline.
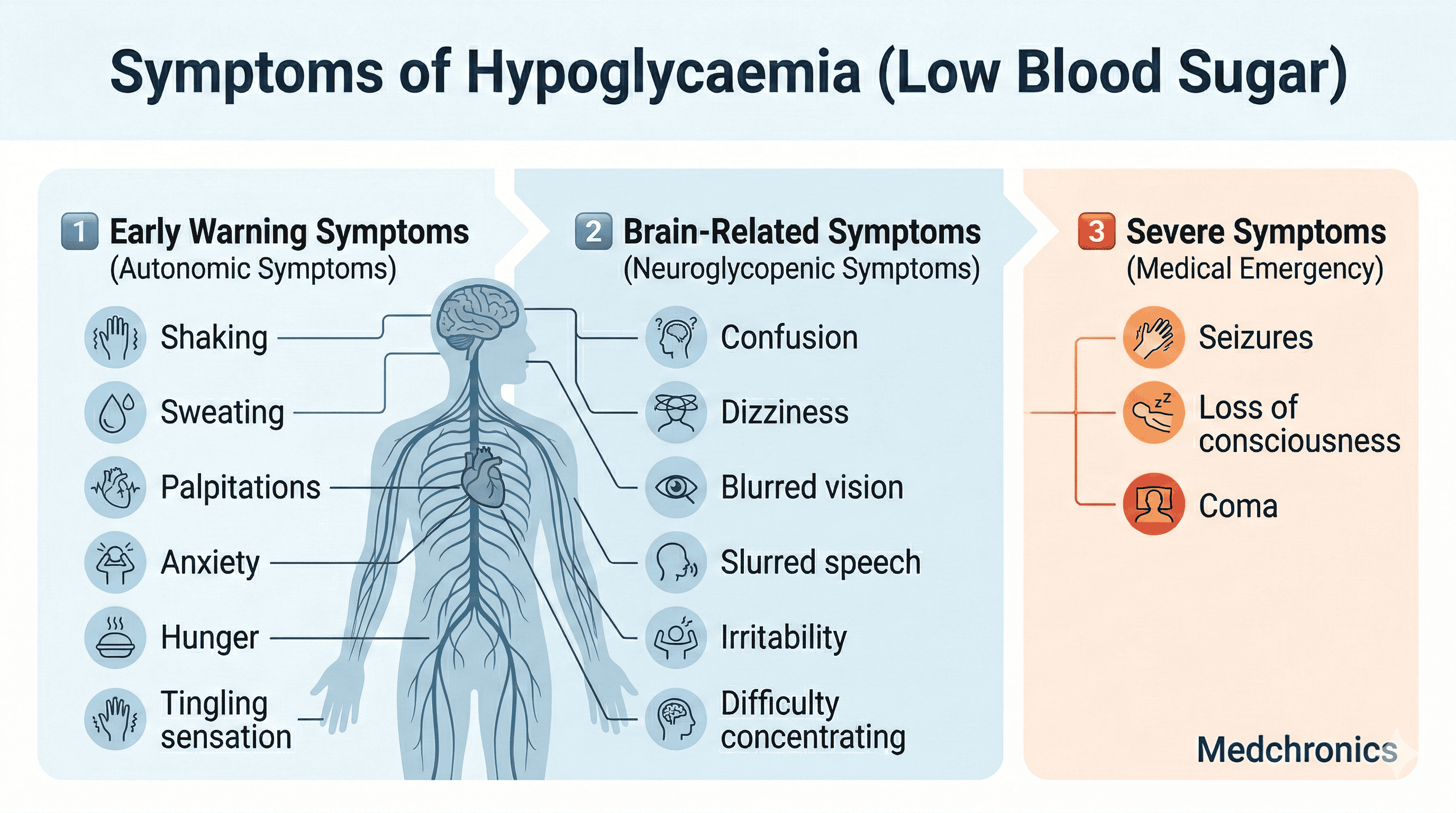
Autonomic (Early) Symptoms:
- Shaking
- Sweating
- Palpitations
- Anxiety
- Hunger
- Tingling sensation
Neuroglycopenic (Brain-related) Symptoms:
- Confusion
- Dizziness
- Blurred vision
- Slurred speech
- Irritability
- Difficulty concentrating
If untreated, symptoms may progress to:
- Seizures
- Loss of consciousness
- Coma
Hypoglycaemia Unawareness: A Silent Risk
Some people, especially those with long-standing diabetes, stop feeling early warning symptoms. This condition is called hypoglycaemia unawareness.
It increases the risk of severe episodes because the person does not get an early alert from the body.
This is why structured glucose monitoring and medication adjustment are essential.
How Is Hypoglycaemia Diagnosed?
Diagnosis involves three components (known as Whipple’s triad):
- Symptoms of low blood sugar
- Confirmed low glucose reading
- Relief of symptoms after glucose correction
Blood Tests
- Capillary blood glucose (glucometer)
- Laboratory plasma glucose
- In rare cases: insulin levels, C-peptide (if tumor suspected)
For doctors and pharmacists, medication history review is critical.
Immediate Treatment: The 15–15 Rule
For conscious patients:
1. Take 15 grams of fast-acting carbohydrates, such as:
- 3–4 glucose tablets
- Half a glass of fruit juice
- 1 tablespoon sugar dissolved in water
2. Regular (non-diet) soft drink
3. Wait 15 minutes.
4. Recheck blood sugar.
After recovery, eat a small snack containing carbohydrates + protein to prevent recurrence.
Severe Hypoglycaemia Management
If the person is unconscious:
- Do NOT give food or liquids by mouth
- Administer glucagon injection (if available)
- Seek emergency medical help immediately
In hospital settings:
- IV dextrose (25–50 mL of 50% dextrose)
- Continuous glucose monitoring
- Electrolyte monitoring
Role of Pharmacists
Pharmacists play a crucial preventive role:
- Counselling patients on insulin timing
- Explaining dose adjustments
- Warning about drug interactions
- Educating about alcohol risks
- Teaching proper glucometer use
Community pharmacists are often the first healthcare contact during mild episodes.
Role of Doctors
For clinicians, management includes:
- Reviewing insulin regimens
- Adjusting sulfonylurea doses
- Identifying high-risk patients
- Considering continuous glucose monitoring (CGM)
- Evaluating recurrent unexplained episodes
Personalized glycaemic targets are important — especially in elderly patients.
Long-Term Prevention Strategies
1. Regular Monitoring
Frequent glucose checks reduce unexpected episodes.
2. Meal Consistency
Avoid skipping meals after insulin.
3. Exercise Planning
Adjust insulin or carbohydrate intake before intense activity.
4. Alcohol Awareness
Alcohol can cause delayed hypoglycaemia, especially overnight.
5. Medication Review
Some drugs increase risk — regular review prevents complications.
Special Populations
Elderly Patients
Higher risk of severe episodes due to:
- Impaired awareness
- Multiple medications
- Cognitive decline
Children
Symptoms may appear as irritability or unusual behaviour.
Pregnant Women
Tighter glucose control increases risk; close monitoring required.
When Should You Seek Medical Help?
Immediate care is needed if:
- Repeated episodes occur
- Loss of consciousness happens
- Seizures occur
- It happens without clear cause
Frequent low sugar episodes indicate that treatment adjustment is necessary.
Why Hypoglycaemia Matters More Than You Think
Many people fear high blood sugar, but severe low blood sugar can be equally or sometimes more dangerous in the short term.
Repeated episodes may:
- Increase cardiovascular risk
- Cause cognitive decline
- Reduce quality of life
- Create fear of insulin therapy
Balanced glucose control is the goal — not just low numbers.
Frequently Asked Questions
Q. Is hypoglycaemia always caused by diabetes?
No. Although most cases occur in diabetic patients, non-diabetic causes exist.
Q. Can hypoglycaemia be life-threatening?
Yes, especially if severe and untreated.
Q. Is 70 mg/dL always dangerous?
Not always, but it is a warning level that requires attention.
Q. Can hypoglycaemia happen during sleep?
Yes, especially in insulin-treated patients.